

By Don Sadler
The health hazards of surgical smoke to patients and perioperative personnel have been well-documented. In fact, the U.S. Occupational Safety and Health Administration’s (OSHA) first alert about the potential dangers of surgical smoke was issued more than 35 years ago.
However, OSHA never formulated regulations requiring hospitals and ASCs to eliminate surgical smoke plume. So, the focus turned to state legislatures instead.
Surgical Smoke Legislation is Spreading
The good news is that the drive to get surgical smoke evacuation legislation passed in more states is picking up steam. In October, California became the most recent state to pass legislation requiring health care facilities to use all tools feasible to remove surgical smoke plume from the operating room.

There are now 15 states with surgical smoke evacuation legislation on the books. Each year, approximately 10 state legislatures consider surgical smoke legislation, and legislation has been passed in five states each of the past two years.
The following states have now passed surgical smoke legislation: Arizona, California, Colorado, Connecticut, Georgia, Illinois, Kentucky, Louisiana, Missouri, New Jersey, New York, Ohio, Oregon, Rhode Island and Washington. In addition, legislation is currently under consideration in six states: Florida,Massachusetts, North Carolina, Pennsylvania, Texas and West Virginia.
 Richard Howard, North America sales manager with I.C. Medical, believes that surgical smoke legislation is important because it is often a precedent for requiring smoke evacuation compliance by health care facilities.
Richard Howard, North America sales manager with I.C. Medical, believes that surgical smoke legislation is important because it is often a precedent for requiring smoke evacuation compliance by health care facilities.
“The use of smoke evacuation modalities has largely been at the discretion of the surgeon or the willingness of management to make them readily available,” says Howard. “Legislation is helping set the precedent that the use of smoke evacuation modalities is no longer a choice, but a requirement. This is putting all stakeholders – including nurses, hospital management and surgeons – on the same page.”
The Association of periOperative Registered Nurses (AORN) has been active in helping get surgical smoke legislation passed at the state level, says Jennifer Pennock, AORN’s associate director of government affairs.
“AORN has concentrated on legislation at the state level to effect change and implement this critical workplace safety provision for as many OR nurses and their colleagues as quickly as possible,” says Pennock.
During a national petition drive in 2021, AORN collected thousands of signatures for a petition urging OSHA to issue regulations requiring worker and patient protections from harmful surgical smoke.
“Since then, we have had numerous meetings with OSHA to discuss actions the agency may take to raise awareness of the workplace hazards of surgical smoke and encourage the use of surgical smoke evacuation systems,” says Pennock.
Pennock adds that surgical smoke legislation is necessary because while many agencies recognize the hazards of surgical smoke and a few even go on to recommend evacuation, there are no national or statewide enforceable requirements for the evacuation of surgical smoke.
“Many surgical facilities evacuate smoke during some procedures, but few evacuate consistently during all smoke-generating procedures,” says Pennock. “Nurses have little control over whether they are assigned to a smoking or non-smoking operating room.”
Pennock notes that restaurant staff and flight attendants are now safe from cigarette smoke, while offices and most public spaces are now smoke-free.
“Nurses and surgical team members deserve the same protection,” she says.
State-by-State Efforts
Ahnyel Burkes, DNP, RN-BC, NEA-BC, was active in getting surgical smoke legislation passed in Louisiana last year.
“Surgical smoke exposure could fall under the general duty clause, which states that employees should be protected at work, but there needs to be specific laws and requirements,” she says. “This is why you’re witnessing a state-by-state effort to get surgical smoke laws passed.”
According to Burkes, the Louisiana law defines surgical smoke plume as “the byproduct of using heat-producing equipment on tissue during surgery.” The law requires licensed health care facilities that perform surgical procedures using heat-producing equipment to adopt and implement policies for a surgical smoke plume evacuation plan to mitigate and remove the surgical smoke plume.
“Compliance with the law will be verified by the Louisiana Department of Health through onsite surveys that are specific to surgical services, full licensing surveys, full recertification surveys and complaint surveys if allegations specific to surgical services are alleged,” says Burkes.
Burkes lays out the playbook for getting surgical smoke legislation passed at the state level. It starts with gathering research about the negative impacts of surgical smoke, along with support from content experts like AORN.
“Next is socializing the issue with other nursing groups to gain support, such as the Louisiana State Nurses Association, which later spearhead the effort,” she says.
Existing legislation in other states was reviewed and meetings with stakeholders who might be impacted by the bill were held next, followed by finalization of the bill’s language.
“Then, we gathered letters of support from other organizations and attended committee meetings to testify in support of the bill, bringing along content experts while simultaneously organizing grassroots support,” says Burkes.
Brenda C. Ulmer, RN, MN, CNOR, was instrumental in getting surgical smoke legislation passed in Georgia in 2022. “I’m very optimistic that our legislation will have positive long-term effects in Georgia,” she says. “In fact, I think we’re already seeing this.”
Ulmer tells the story of talking to a medical student during her annual physical exam: “The student asked about my background and I told him I did education on electrosurgery and surgical smoke. He said, ‘You know, there’s a law in Georgia about surgical smoke now.’ I just chuckled and told him that yes, I did know about it.”
“In my mind, this is proof positive that a practice change has definitely occurred,” says Ulmer.
Unfortunately, surgical smoke legislation in Texas suffered a setback recently when two bills passed hearing and made it to the floor for a vote.
“However, time ran out before voting could commence and the bills died on the floor,” explains J.D. Buchert, M.Ed., MS, MSN(s), RN, CNOR, the president of the Texas Collaboration of periOperative Registered Nurses (TCORN).
Buchert says this is the closest these bills have ever gotten to passage.
“My biggest reason for advocating so heavily about surgical smoke legislation is simple: Because it’s the right thing to do,” he says. “As perioperative nurses, we want to help save lives and not be put in danger while doing it.”
TCORN is now working with AORN to get surgical smoke evacuation placed in the state regulatory process.
“We’re trying to maintain the verbiage of both bills and the integrity of the surgical smoke evacuation focus in the regulations,” says Buchert. “While our fingers are crossed that this regulation passes, we will also continue to pursue the bills to make this state law.”
According to Pennock, surgical smoke legislation tends to be most successful in states with strong grassroots advocates who are committed to working on policy advocacy for multiple years and through legislative sessions.
“To lay the groundwork for successful legislation, it’s important to engage with stakeholders early in the process,” says Pennock. “It’s also important to identify a strong bill sponsor in the House or Senate who will throw their political influence into the success of the bill, and to gain support from state nurses’ and hospital associations.”
Why Surgical Smoke is So Dangerous
Approximately 90% of all surgical procedures generate surgical smoke and up to half-a-million health care workers are exposed to surgical smoke each year. The average daily impact of surgical smoke on the surgical team is the equivalent of inhaling the smoke of up to 30 unfiltered cigarettes.
Surgical smoke contains more than 150 hazardous chemicals and carcinogenic and mutagenic cells. “It contains toxic gases and vapors such as benzene, hydrogen cyanide, formaldehyde, bioaerosols, dead and live cellular material, blood fragments and viruses,” says Pennock.
In addition to the danger to health care workers, surgical smoke can also cause cancer cells to metastasize in the incision site of patients having cancer removal surgery. Babies born by C-section breathe in their parent’s surgical smoke at birth.
While patient exposure to surgical smoke is short-term and relatively low risk, surgeons and other OR staff may be exposed to surgical smoke daily. At high concentrations, this smoke may cause ocular and upper respiratory tract irritation.
In a study reported in the Journal of Clinical Nursing in 2016, 49% of nurses and 58% of surgeons reported experiencing headaches, 40% of nurses and 42% of surgeons reported watery eyes, and 49% of nurses and 28% of surgeons reported coughing due to exposure to surgical smoke.
Nurses and surgeons also attributed sore throat, nausea, drowsiness, dizziness, sneezing, rhinitis and bad odors absorbed in the hair to surgical smoke. In fact, perioperative nurses report twice as many respiratory problems compared to the general population.
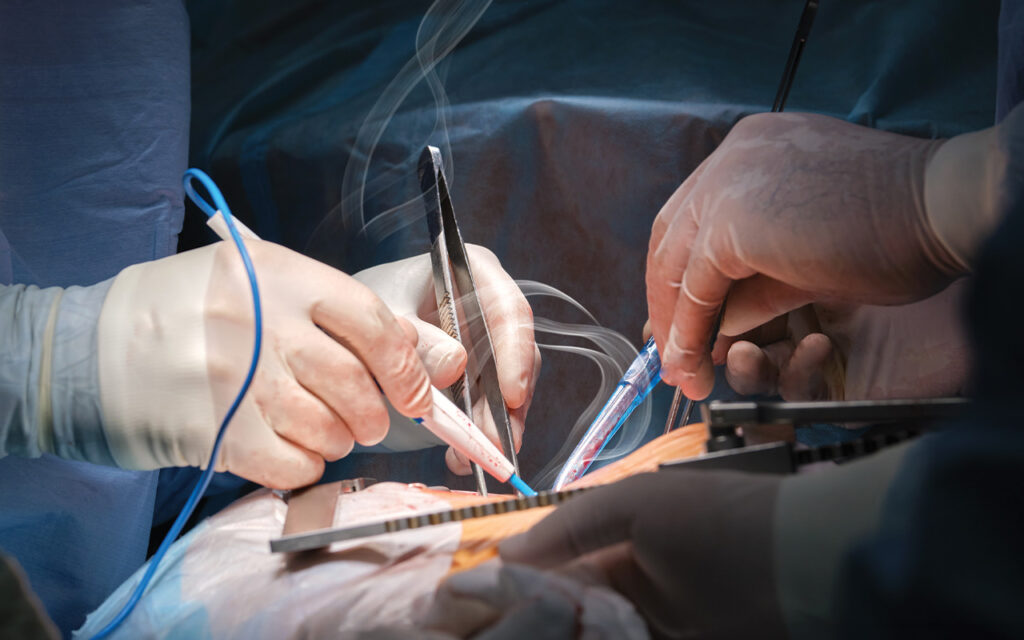
The best solution to these problems is to safely and effectively eliminate surgical smoke by using a smoke evacuator device. “Evacuating the smoke from its source is vital,” says Howard. “We must effectively capture all of the plume directly from the source.”
For surgical procedures generating a large amount of plume, a dedicated smoke evacuator, equipped with a ULPA filter, will be used. “Either a smoke evacuation pencil or handheld wand tubing will be connected to the smoke evacuator and positioned near the source of smoke generation,” Howard explains.
For procedures generating a nominal amount of plume, the hospital wall suction system, equipped with a ULPA filter installed in-line, will be used. “A smoke evacuation pencil, pencil tubing adapter or handheld wand tubing will be connected to the suction device and positioned near the source of smoke generation,” Howard explains.
Used filters with captured surgical smoke are disposed of as hazardous waste.
A Grassroots Movement
With the current momentum, Ulmer is optimistic about the passage of more surgical smoke evacuation laws across the country.
“These are grassroots movements led by nurses,” she says. “I believe this is a powerful message to nurses as they work to improve the operating room environment for health care workers and patients.”
AORN provides ongoing education about surgical smoke, including the AORN Go Clear program. To learn more visit https://www.aorn.org/education/education-for-facilities/surgical-safety-center-of-excellence/go-clear-awards.






