

By Nancymarie Phillips, PHD, RN, RNFA, CNOR(E)
Safe Patient Care
Safe and effective patient care is the core of perioperative practice. AORN (The Association of periOperative Registered Nurses), the professional organization of perioperative RNs, published the Perioperative Patient Focused Model, which recognizes that “there is nothing more important to the practicing perioperative nurse than his or her patient.”1 Publications such as AORN’s Guidelines for Perioperative Practice, articles in peer-reviewed journals, research, safe practice guidelines, and tool kits are valuable resources for safe patient care; however, failures in patient care processes and systems still occur and can result in errors in patient care.1 These occurrences and “near misses” can harm patients. When the error is detected before the care or treatment is administered (a “good catch”), patient harm is avoided. Sometimes, the care is administered but does not appear to cause patient harm.
OnCourse Learning guarantees this educational activity is free from bias. The planners and authors have declared no relevant conflicts of interest that relate to this educational activity. See page 40 to learn how to earn CE credit for this module.
The goal of this continuing education program is to provide perioperative nurses, surgical technologists, and pharmacists with information about the challenges of and effective strategies for medication and solution labeling in the perioperative setting. After studying the information presented here, you will be able to:
- Discuss the intent of The Joint Commission’s National Patient Safety Goal NPSG.03.04.01 involving labeling medications and solutions on and off the sterile field
- Identify the challenges for safe medication administration unique to the perioperative environment
- Describe strategies for effective medication and solution labeling on and off the sterile field
Everyone is familiar with the adage, “What you see is what you get.” But can healthcare professionals rely on it when it comes to safe medication administration in the perioperative setting — or should “Looks are deceiving” be their motto?
This module explores patient safety goals and strategies for effective medication and solution labeling on and off the sterile field in the perioperative environment. Perioperative healthcare professionals and pharmacists must be knowledgeable about these concepts so they can promote patient safety and desirable outcomes.

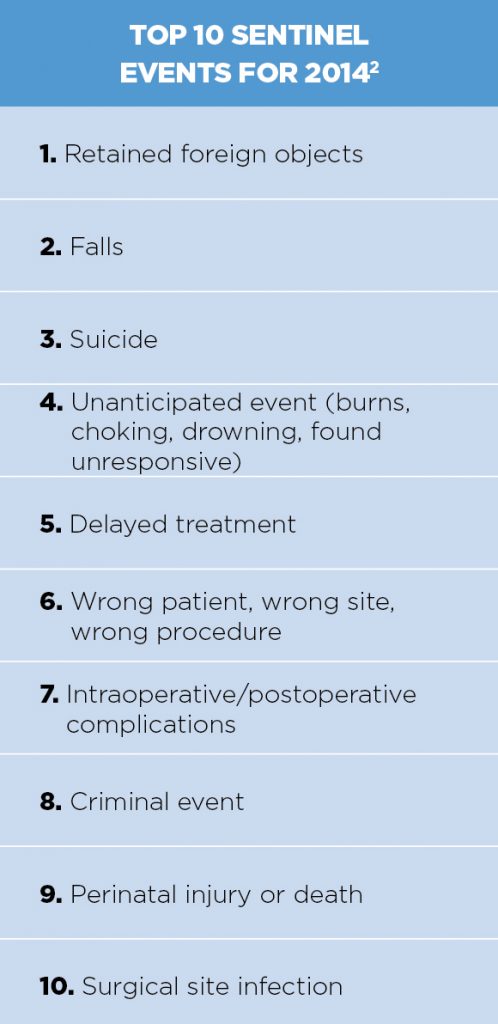
Unfortunately, sometimes the care, treatment, or medication is administered erroneously, resulting in temporary or even long-term harm to the patient. These negative outcomes, including medication errors, receive national attention when they become one of The Joint Commission’s (TJC) sentinel events. The Patient Safety Advisory Group (formerly the Sentinel Event Advisory Group), appointed by TJC in 2002, reviews and investigates reported sentinel events by performing root cause analyses. Medication errors are reportable sentinel events. Fortunately, national attention to the administration and management of medications was not one of the top 10 sentinel events reported for 2014. A significant reduction in medication errors is noted. Sentinel event data compiled from 1995 to 2016 can be viewed at https://www.jointcommission.org/assets/1/18/Summary_4Q_2016.pdf.
The Institute of Medicine’s 1999 report on medical errors, To Err Is Human: Building a Safer Health System, has made patient safety initiatives a priority for healthcare organizations and government agencies. In 2002, AORN launched the Patient Safety First campaign to reduce errors in surgical settings and create resources to help perioperative clinicians provide safe patient care. Specific practices include correct patient and surgical site verification and surgical counts, as well as medication safety, which can be found in the AORN Guidelines for Perioperative Practice.
TJC first established its National Patient Safety Goals (NPSGs) in 2003, and the NPSGs continue to influence patient care. Goal 3 (improve the safety of using medications) addresses safe medication and solution administration. Perioperative care areas must meet the three specific requirements of Goal 3:
- Label any medication that is not in its original container and place it into a syringe, cup, or basin
- Know the medications the patient currently takes, especially blood thinners
- Document and report medications the patient takes at home
- The complete list of TJC patient safety goals for 2017 can be found at https://www.jointcommission.org/standards_information/npsgs.aspx.
NPSG.03.04.01. The NPSGs are intended to develop standards and directions for practice to create a national movement for patient safety. NPSG.03.04.01 requires clear labeling for medications and solutions that have been removed from their original containers or packaging and transferred to other containers for use on and off the sterile field by a person other than the preparer. This requirement applies to the entire perioperative environment and procedural components of any patient care setting in which operative or invasive procedures are performed, including medications used by anesthesia providers. The practice of using labels on all cups, basins, and delivery devices has been effective in decreasing the incidence of medication errors in the OR.3 Most sterile custom set-up packs contain blank labels and a pen or preprinted labels for use in the sterile field.
 Characteristics of Perioperative Settings
Characteristics of Perioperative Settings
A healthcare facility is a complex environment with many departments and patient care units. In general, facilities are similar in their management of patient care; however, the OR is a different and separate entity with unique nuances and distinct management processes and methods of delivering patient care.
OR patient populations span the age continuum, from neonates to geriatric patients. It is common to care for pediatric and adult patients in one day, whether within one or several surgical specialties. Age-specific medication information and guidelines should be readily available.4
In many organizations, the perioperative continuum of care is the most involved, with many critical factors, steps, and processes influencing patient outcomes. Several departments and caregivers hand off the perioperative patient in a short period of time. Communication — whether verbal, written or electronic — lends itself to medication error if nonstandard or easily misinterpreted abbreviations are used. Abbreviations should be avoided in medication orders and documentation.5 TJC has published a “Do not use” list of abbreviations that can be printed and posted in the patient care divisions.
Generally, the medication process in the OR involves the prescribing physician, the preparing and dispensing pharmacy, the circulating nurse, and the scrub person, who is the final check before the medication is administered from the sterile field. Other variables, such as the OR environment, staff availability, and administrative support impact the effectiveness of the medication and the solution safety initiative.3
OR Environmental Conditions
Many surgical procedures require that room lights be dimmed or turned off. The X-ray view box, a lamp on the anesthesia cart, surgical spotlights, or a lighted workspace provides alternative or indirect lighting. Visibility is compromised, especially for reading medication labels and preparing and managing medications and solutions on and off the sterile field. The workspace in the circulating nurse’s area can be small and cluttered with equipment and retrofitted computers and keyboards.6
From “patient-in” to “patient-out,” the OR is a busy area. Conversations take place between team members. Distractions and interruptions are common. During the surgical procedure, the circulating nurse manages multiple priorities of the patient, anesthesia provider, surgeon, and scrub person while still monitoring the sterile field. The circulating nurse works in a constant state of anticipation of who might need what next.6
Staffing
Adequate staffing with the appropriate skill mix and assignments is important for safe patient care. The current realities of short staffing, temporary and contract staff, and novice team members create challenges. Complex or multiple specialty procedures requiring additional staff create further demands.3,6
Additional staffing is beneficial during complex or multiple specialty procedures with extensive setup and during the initial patient positioning, prepping, and incision time. Typically, these procedures have several priorities for the patient, anesthesiology provider, and surgeon. A second circulating nurse can work exclusively with the scrub person to prepare, dispense, and label the medications or solutions.6 The work schedule should be managed to avoid extended work hours since fatigue contributes to medical errors.
OR Time Management Influences
Time is an important indicator when evaluating performance and productivity in the OR. Shorter procedure times, quicker turnover, increased case volume, and total procedure minutes are monitored. A sense of “faster, faster, faster!” exists. Certain eye procedures take little time to perform, but use multiple medications in the sterile field.6 Some procedures, such as Dilatation and Curettage (D&Cs) and arthroscopies, can leave the team with the feeling the case is over before it starts. It is an environment of rapid interventions. The margin for error is great, especially concerning medications and solutions in the OR.
Medication Orders
The medication process involves:
- Prescribing (a physician’s order)
- Processing the order (transcribing and documenting)
- Preparing the medication or solution
- Dispensing
- Administering the medication to the patient
- Monitoring and documenting the effect of the medication
In the OR, the preference card has long been viewed as the primary source for the physician’s written medication orders and as a “standing order.” The circulating nurse has the professional responsibility to check the medication needs with the surgeon before the case is set up.6 The supplies needed might be different. Medications are sometimes listed on the preference card with options (e.g., if local, use medication “A”; if general, use medication “B”). If preference cards are used, the circulating nurse should update any changes by initialing and dating the revision.6
The relationship of preference cards to medication errors is cause for concern. Information on preference cards can be outdated, incomplete, or inaccurate. Inconsistent nomenclature (e.g., generic vs. brand name), abbreviations, unclear dosage, and concentration calculations should be clarified with the surgeon before the surgical procedure begins.6 Validation of the medications can be incorporated into the time out procedure as part of the available supplies before the incision is made. This process is important in the prevention of medication errors.
Medication orders may be given verbally in the preoperative holding area or during an OR procedure. Medication orders given verbally in the OR are a potential source of error. Masks can muffle speech, the surgeon may have an accent, several conversations are often underway simultaneously, music may be playing, surgical equipment and monitors create ambient noise, and the circulating nurse is usually juggling priorities. Verbal orders should be repeated back and documented as soon as possible, with the physician signing the order. (This can be a problem if the surgeon is scrubbed at the time the order is given.) The surgeon must sign the medication order after the surgical procedure is completed.3,6
 Medication Preparation
Medication Preparation
The perioperative setting creates concern about the safe preparation of medication concentrations. Several people handle medications and solutions dispensed to the sterile field before the surgeon administers them. The circulating nurse may need to obtain and reconstitute a drug to a specific concentration before it can be used in the sterile field. The correct diluent and amount (sterile saline or sterile water) is as important as is the correct drug. The circulating nurse’s knowledge of surgical pharmacology is an important factor in preventing medication errors.6
One surgical procedure can require the preparation and mixing of several medications and solutions. Clear, complete, and accurate instructions and conversion charts for the dosage and concentration calculations (including age-specific information) are critical. The pharmacy is responsible for preparing specialty medications and solutions, such as 4% cocaine hydrochloride for otorhinogologic cases. The circulating nurse cannot mix this preparation and must obtain it from the pharmacy. Other drugs are stored in stock or in a machine referred to as automated machines like Pyxis dispenser. The dispensing machine is activated by using the ID number of the circulating nurse and the patient’s ID number.5 This is another method of documenting a drug for patient use.
Medication Dispensing and Administration
Unique to the OR is the additional team member, the scrub person (who may be an RN or a surgical technologist). After confirming the correct drug, dose, and expiration date, the circulating nurse aseptically dispenses the medication or solution to the sterile field where the scrub person immediately labels the receptacle (cup or basin) and delivery device under sterile conditions. The label should at a minimum include the drug’s name and strength.6 Some facilities require the scrub person’s initials. When the drug is handed to the surgeon, the scrub person repeats the name and strength of the drug. The delivery device (syringe) is premarked by the manufacturer with dosage measurement increments for the surgeon’s use. The surgeon returns the used syringe to the scrub person, who in turn reports the amount used to the circulating nurse.6 The nurse documents the amount used in the patient’s OR record.
All original drug containers from the pharmacy are retained by the circulating nurse until the end of the case as validation of correct medication preparation and usage. The systems in place for drugs used in the sterile field contribute to the safety of medication administration in the OR.
Medication Intensive
The OR is medication intensive. It is common for several medications to be used during one surgical procedure. The procedure may require several categories of medications — for example, topical and local anesthetics, contrast media, dyes, gases, antibiotics, anticoagulants — as well as solutions (plain or with additives) administered by various routes (topical, injection, infusion, or irrigation).6 These preparations are delivered by the sterile team at the field. Other forms of these drugs are administered by the anesthesia provider in concert with the surgeon. Surgical pharmacology becomes very complicated when determining medication safety and preventing drug interactions.
In addition, high-alert medications such as heparin and epinephrine are common in the OR. Once on the sterile field, “look-alike” concerns extend beyond similarities in medications’ names and appearance. Most medications and solutions are clear and look similar, such as irrigation solutions (e.g., saline, sterile water, and lactated ringers) and local anesthetics, whether plain or with additives. Specialty drugs and solutions prepared by the pharmacy may be tinted pale contrast colors for easy identification but nonetheless they should be clearly labeled and these labels checked prior to administration. For example, 4% cocaine hydrochloride is often tinted light green and provided only in 4 to 5 mL increments for topical use in nasal surgery.6
Safety Goals
Perioperative nurses assume the role of the patient’s advocate during the perioperative experience; as the patient’s advocate, the perioperative nurse is many times the most significant barrier to adverse events.1,3,6 With patient safety as the priority, the RN critically assesses every activity and intervention as safe practice. Professional responsibilities require the RN to use best practices and to be aware of changes in practice, as well as knowing the organization’s patient safety initiatives. Patient safety goals provide the RN with an opportunity to be a patient safety leader.
Administrative Support
Essential to quality or process improvement is the support and ongoing follow-up from an organization’s leadership. Managers provide leadership for a collaborative, multidisciplinary systems approach to improve processes. They also play an important role in establishing safe practice protocols and identifying necessary core competencies to create highly reliable patient care. This collaborative teamwork fosters mutual respect, with each practitioner knowing his or her role, understanding the roles of fellow caregivers, and having a sense of responsibility and accountability to teammates. Leadership must provide the resources that staff need to ensure this culture of safety.3,6 These resources may include:
- Staffing that provides the appropriate number, skill mix, and assignments
- Time for education and training, case setup, and medication preparation
- A safe work environment with reduced distractions and interruptions, as well as appropriate lighting and work areas
- A nonpunitive culture in which reporting of errors is a routine professional responsibility
- Information for increased awareness, quality data, and education and training
- Tools and supplies that support safe practice and adherence to policies, including labels and markers, and alternative lighting for work areas on and off the sterile field
Label Information
Unlabeled medications are unidentifiable. Transferring medications to the sterile field without labeling is an unsafe practice that neglects basic principles of safe medication management. NPSG.03.04.01 mandates labeling for medications on and off the sterile field. Label information must include a medication’s name and strength as well as amount when medications are mixed (as with antibiotic irrigations, tumescent and heparin solutions, and epinephrine). The unit of measure — percent, grams, milliliters, or units — must be recorded along with the date the medication is prepared.
An expiration date is applicable when the medication is not used within a certain time period designated by the manufacturer or if a specific time limit after reconstitution exists. Original containers and delivery devices must be kept in the OR for verification until the procedure is completed.6 Anything in unlabeled containers must be disposed of immediately. The only exception to labeling is when the medication is immediately (no intervening steps or functions before administration) used or disposed of.
Label Quality
Labels are placed on containers, including syringes, medicine cups, pitchers, bulb syringes, and solution bags made of metal, glass, and plastic. The labels are subjected to a wet field for several hours; therefore, labels should be evaluated for the following:
- Adhesive durability
- Ink that resists smudging when wet or handled often
- Adequate size to allow all required information to be legible and clearly visible
- Adaptability to fit on a variety of shapes and sizes of containers
- Cost effectiveness and availability
Several labeling systems are available. Kits and custom packs include pens with permanent ink and labels that are color coded, preprinted, or custom printed to meet a hospital’s needs.
 Transferring to a Sterile Field
Transferring to a Sterile Field
When two or more qualified people are preparing and administering medications and solutions in the intraoperative setting, they must communicate clearly when transferring the medications and solutions to the sterile field. They must verbally and visually confirm the information on the medication label. To maintain consistency with counting policies, an RN should be one of the people involved. When one person both prepares and administers the medication immediately, the two-person verification is not required.6 If the medication is prepared but not given immediately, labeling is required.
Labeling. Medications must be labeled immediately when they are received on the sterile field. Even if only one medication or solution is on the sterile setup, it must be labeled. An effective strategy is the use of preprinted labels, which can be included in the custom pack as well as in separate sterile packaging. Prelabeled containers such as bowls, basins, and syringes are not acceptable since the risk exists for a different medication or solution to be transferred to the container. Label one medication at a time to prevent mislabeling and always double check your work.
Consistent labeling protocols must be practiced throughout the department in all specialty services. NPSG.03.04.01 focuses on medications that are removed from their original containers, that are both on and off the sterile field, and that are intended to be administered to the patient during the procedure. Solutions with additives, such as electrolytes, antibiotics, and epinephrine, that are delivered from the original container by a device such as an irrigation pump must also be clearly labeled. Labeling is required for “one-person scenarios” (i.e., when one person prepares the medication or solution but does not administer it immediately).
Verification on the field. When passing a medication or solution to the surgeon, the scrub person must say the medication or solution name and strength out loud.6 Many times, the surgeon cannot take his or her focus from the immediate surgical field, has asked for several items at a time, or may be continuing a discussion with other team members. The surgeon must confirm the name and strength of the medication or solution as well.
Communication
Another unique aspect of patient care in the OR is that the primary scrub person and circulating nurse can transfer responsibilities of direct and indirect patient care activities. Procedures and protocols must be established for communication of medication information during temporary relief for turnover, case setup, and breaks, and during permanent relief for patient handoffs at change of shift and to specialty teams. Information discussed by the entering and exiting team members must include the medication or solution name, strength, concentration, and amount administered. It is important to discuss medications used during the procedure in the postanesthesia handoff report.7
NPSG.03.04.01 provides a focus for safe medication administration in perioperative practice. A review of the facility’s medication administration process will determine revisions and resources required for safe practice policies and procedures. Having the perioperative team use consistent medication labeling and verification processes as the standard of practice helps reduce medication errors.
Editor’s Note: Cynthia K. Halvorson, MSN, RN, CNOR, the original author of this educational activity, has not had an opportunity to influence the content of this version.
OnCourse Learning guarantees that this educational activity is free from bias.
Nancymarie Phillips, PhD, RN, RNFA, CNOR, is a tenured professor and the head of the perioperative education department at Lakeland Community College in Kirtland, Ohio. Her curriculum includes perioperative nursing, registered nurse first assistants, and surgical technology. She has 40 years of experience in perioperative nursing and is the author of several texts and articles about perioperative practice. The author has declared no relevant conflicts of interest that relate to this educational activity.
References
1. Perioperative patient-focused model. In: Guidelines for Perioperative Practice. Denver, CO: AORN; 2015: 4.
2. Punke H. Top 10 sentinel events in 2014. Becker’s Infection Control & Clinical Quality. June 4, 2015. http://www.beckershospitalreview.com/quality/top-10-sentinel-events-in-2014.html. Accessed May 10, 2016.
3. Landers R. Reducing surgical errors: Implementing a three-hinge approach to success. AORN J. 2015;101(6):657-665. doi: 10.1016/j.aorn.2015.04.013.
4. Wallace J, Paauw DS. Appropriate prescribing and important drug interactions in older adults. Med Clin N Am. 2015;99(2):295-310. doi: 10.1016/j.mcna.2014.11.005.
5. Collard B, Royal A. The use of abbreviations in surgical note keeping. Ann Med Surg (Lond). 2015;4(2):100-102. doi: 10.1016/j.amsu.2015.03.008.
6. Phillips NM. Berry and Kohn’s Operating Technique. 12th ed. St. Louis, MO: Elsevier; 2012.
7. Petrovic MA, Aboumatar H, Scholl AT, et al. The perioperative handoff protocol: evaluating impacts on handoff defects and provider satisfaction in adult perianesthesia care units. J Clin Anesth. 2015;27(2):111-119. doi: 10.1016/j.jclinane.2014.09.007.
How to Earn Continuing Education Credit
1. Read the Continuing Education article.
2. Go online to ce.nurse.com to take the test for $12. If you are an Unlimited CE subscriber, you can take this test at no additional charge. You can sign up for an Unlimited CE membership at www.nurse.com/unlimitedCE for $49.95 per year.
Deadline: Courses must be completed by 6/30/2018.
3. If the course you have chosen to take includes a clinical vignette, you will be asked to review the vignette and answer 3 or 4 questions. You must answer all questions correctly to proceed. If you answer a question incorrectly, we will provide a clue to the correct answer.
4. Once you successfully complete the short test associated with the clinical vignette (if there is one), proceed to the course posttest. To earn contact hours, you must achieve a score of 75%. You may retake the test as many times as necessary to pass the test.
5. All users must complete the evaluation process to complete course. You will be able to view a certificate on screen and print or save it for your records.
Accredited
In support of improving patient care, OnCourse Learning is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
OnCourse Learning is also an approved provider by the Florida Board of Nursing, the District of Columbia Board of Nursing, and the South Carolina Board of Nursing (provider #50-1489).” OnCourse Learning’s continuing education courses are accepted by the Georgia Board of Nursing. OnCourse Learning is approved by the California Board of Registered Nursing, provider #CEP16588.
ONLINE
Nurse.com/CE
You can take this test online or select from the list of courses available.
Prices subject to change.
Questions
Questions or for a complete listing of our courses:
Phone: 800-866-0919
Email: ce@nurse.com
Clinical Vignette
The relief team for the primary ophthalmology group arrives as the surgery concludes and the eye patch is placed on the surgical patient. The relief team asks the primary team to immediately take its break since they have a full relief schedule. The relief RN transfers the patient to the PACU and then completes the next case setup for cataract extraction with lens implantation and trabeculectomy with the relief scrub person. Expected case setup time is seven minutes; the case will take roughly 20 minutes to complete.
The medications are prepared and transferred to the sterile field using needle gauge and syringe size combination for identification of the medications and solutions. The balanced saline solution (BBS), an isotonic irrigating solution to maintain pupil dilation and keep the eye moist, is hung on the phacoemulsification unit. Several milliliters of the BSS are flushed through the phacoemulsifier tubing and the hand piece into a glass medicine cup to prime the unit and hand piece. The relief circulating nurse pours 500 mg of vancomycin (Vancocin) in 10 mg of normal sterile saline into a second glass medicine cup while the scrub person prepares the Mayo stand instrumentation. The relief scrub person prepares the medications and solutions, matching syringe size and needle gauge for identification, including a 3-cc syringe filled with BSS from the glass medicine cup to avoid opening another BSS sterile dose bottle (15 mL) at the end of the procedure. This syringe is placed between the medicine cups on the back table. The relief scrub person places the glaucoma drainage device implant into the vancomycin mixture in the second medicine glass until the surgeon is ready to implant the device.
The primary team returns from break as the surgical prep is completed. Since the primary team and surgeon have a long-term working relationship, the surgeon rarely needs to ask for the next instrument, medication, or solution during procedures.
At the end of the cataract procedure, the surgeon seals the surgical wound and injects the incision with BSS from the 3-cc syringe prepared during the case setup. As the surgeon returns the syringe to the Mayo stand, the primary scrub person realizes it is unclear whether the syringe was filled from the medicine glass containing BSS or the one containing vancomycin. Since antibiotics are toxic when injected into the eye — and vancomycin has a long half life in normal eyes — a retinal ophthalmologist is called to the OR to perform emergency management with aggressive BSS lavage.
The trabeculectomy procedure is not performed because of the emergency situation. Since the patient is at risk for a loss of visual acuity and even blindness, additional postoperative follow-up is required. In addition, the patient requires continued medical management of the glaucoma until it is appropriate to reschedule the trabeculectomy.
1. What is a contributing factor in this medication error?
a. Lack of labeling of medications transferred from the original container to syringes on the sterile field
b. Long-term specialty team working with the surgeon
c. Verbal confirmation of medications as passed to the surgeon
d. Appropriate handoff between the two OR teams
2. Medication errors during surgery resulting from unlabeled secondary containers and syringes on the sterile field are significant for:
a. Obligating any future surgical procedures for the patient to be on an inpatient basis
b. Causing potentially long-term harm to the patient
c. Managing interventions by the anesthesia provider
d. They have no significance beyond the immediate surgical procedure
3. To avoid future medication errors, the ophthalmology service should implement which strategy?
a. Take breaks when there is a delay or at the end of the case schedule
b. Deny operating privileges to the surgeon involved
c. View the incident as a statistical inevitability
d. Label syringes and other containers on the sterile field and conduct a handoff review of medications and amounts given






