

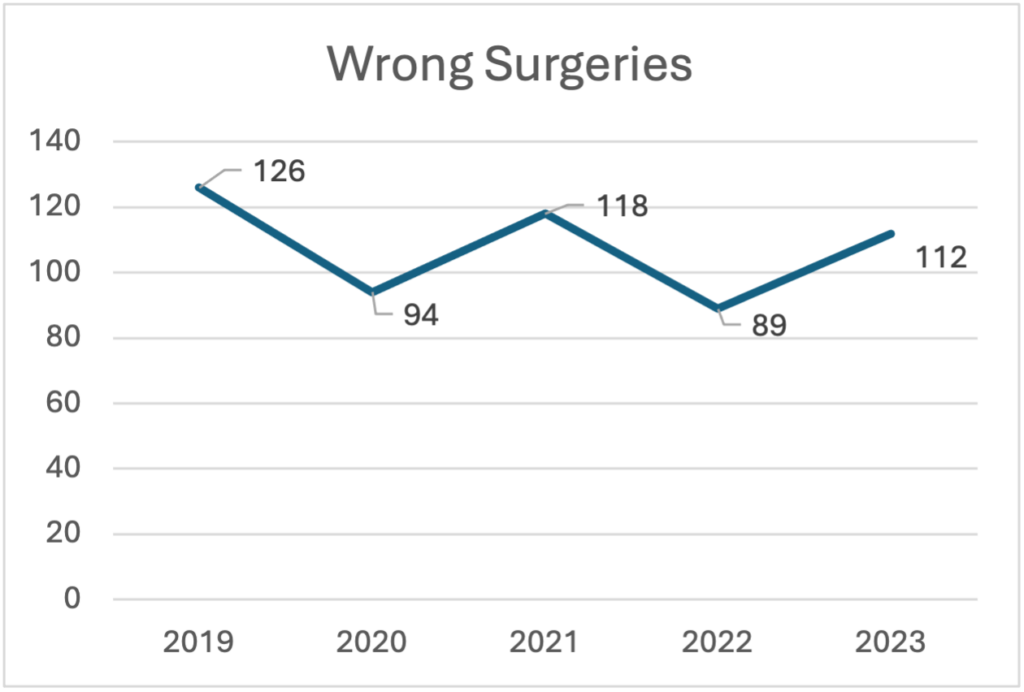
Diagram 1 ( (The Joint Commission, 2024))
By Dawn Whiteside


Dawn Whiteside, DNP, MSN-Ed, RN, CNOR, NPD-BC, RNFA
In May of 2024, the Joint Commission published its annual report regarding sentinel event data for 2023. Reporting sentinel events to The Joint Commission is a voluntary process, which may lead to the conclusion that the actual numbers are significantly higher than reported. (The Joint Commission, 2024) The data reported for 2023 demonstrates a 26% increase in wrong surgeries from 2022 (Diagram 1). Of the 112 wrong surgeries in 2023, the breakdown is as follows: 62% wrong site, 19% wrong procedure, 12% wrong patient and 7% wrong implant. (The Joint Commission, 2024) (The Joint Commission, 2024)
Specific to the perioperative specialty, wrong surgeries encompass surgery or other invasive procedures performed on the wrong person, wrong site or is the wrong procedure. According to the National Quality Forum and the Center’s for Medicare and Medicaid, wrong-site, wrong-procedure and wrong-patient errors are considered never events and sentinel events by The Joint Commission. (Agency for Healthcare Research and Quality, 2006) “The Joint Commission defines a sentinel event as a patient safety event (not primarily related to the natural course of the patient’s illness or underlying condition) that reaches a patient and results in death, permanent harm (regardless of severity of harm), severe harm (regardless of duration of harm).” (The Joint Commission, 2024, p. 3) After a study in 2004 revealed the rate of wrong surgeries to be estimated at 1:113,000 from 1985-2004, the Joint Commission enacted the Universal Protocol. (Agency for Healthcare Research and Quality, 2006)
The three key components of the Universal Protocol include pre-procedure verification, site marking and time-out. The pre-procedure verification is the first gate towards preventing wrong surgeries and includes verifying the correct procedure, for the correct patient, at the correct site with the patient actively involved. This is also the step when all relevant and required documentation is present and accurate. Site marking is the second gate to protect patients and should have patient involvement. Marking the surgical site is required when there is more than one possible location. Site marking should be done by the licensed practitioner, or delegate, be visible after prepping and draping, and include alternative site marking options (armband, etc.) when marking the site is not possible or a patient refuses. The final gate to preventing wrong surgeries is conducting a time-out. The time-out should be a standardized process across the facility. One individual announces the beginning of the time-out process which is when all conversations and distractions cease. All attention is given to the process and all individuals are actively involved. At a minimum the time-out must include the identification of the correct patient, the correct procedure and the correct procedural site. The current standard in most facilities includes additional information like a fire risk assessment, anesthesia considerations and affirmation, introduction of unknown team members, any expected risks to the patient and patient care interventions already implemented (sequential compression devices, blood screening, etc.). “Root cause analyses of [Wrong-Site, Wrong-Procedure, and Wrong-Patient Surgery] WSPEs consistently reveal communication issues as a prominent underlying factor.” (Patient Safety Network, 2019)Prevention efforts must start with a just culture and improved communication. “A just culture focuses on identifying and addressing systems issues that lead individuals to engage in unsafe behaviors, while maintaining individual accountability by establishing zero tolerance for reckless behavior.” (Agency for Healthcare Research and Quality, 2019) The evolution of improving efficiencies in the operating room, like turnaround times, may lead some team members to use shortcuts and skip steps that seem unnecessary. This is commonly referred to as normalized deviance. Effective communication among team members is essential to prevent patient injury. Using a standardized tool like a surgical safety checklist provides a method of communication among all team members to decrease the risk of WSPEs. There are several surgical safety checklists available for use to support the full Universal Protocol procedure. The World Health Organization (WHO) developed a surgical safety checklist in 2009. The Association of perioperative Registered Nurses (AORN) created the Comprehensive Surgical Checklist “using color codes to signify items from the WHO checklist, The Joint Commission Universal Protocol, and areas where the two overlap, the Comprehensive Surgical Checklist offers guidance for preprocedural check in, sign in, time out, and sign out.” (Association of periOperative Registered Nurses, 2024)
As medical professionals, we are very familiar with the phrase “first, do no harm.” If I asked the question where this phrase came from, I am guessing it would be an overwhelming response of “the Hippocratic Oath.” This would have been my response, as well, which is incorrect. Hippocrates, a Greek physician, is credited with this phrase and believed to be by Hippocrates, Of the Epidemics, he wrote “The physician must be able to tell the antecedents, know the present, and foretell the future – must mediate these things, and have two special objects in view with regard to disease, namely, to do good or to do no harm.” (Shmerling, 2020) The nursing equivalent is the Nightingale Oath taken upon graduation from nursing school at many colleges and universities.
Nurses are accountable for their patient’s well-being and are guided by not only their own morale principles but also the American Nurses Association (ANA) Code of Ethics. There are nine provisions within the Code and additional topics within each provision. It is essential that all nurses read and understand the Code. We must live and work by this Code to protect our patients from harm. Within the Code there are specific provision statements related to Respect for Human Dignity, Primacy of the Patient’s Interests, Protection of Patient Health and Safety, and Authority, Accountability, and Responsibility.
Is it possible to get it right? The leading causes of sentinel events include ineffective communication, breakdown in teamwork and inconsistently following policies. (The Joint Commission, 2024) Making improvements to each of these causes should certainly decrease the number of possibilities. Using a surgical safety checklist, following and enforcing safety policies, and working to improve teamwork and communication should be at the forefront of organizational goals. Ultimately, we should never underestimate our capacity to do harm and always focus on preventing patient injury.
References
Agency for Healthcare Research and Quality. (2006, April 26). Universal Protocol for Preventing Wrong Site, Wrong Procedure, Wrong Person Surgery. Retrieved from Patient Safety Network: https://psnet.ahrq.gov/issue/universal-protocol-preventing-wrong-site-wrong-procedure-wrong-person-surgery
Agency for Healthcare Research and Quality. (2019, September 7). Culture of Safety. Retrieved from Patint Safety Network: https://psnet.ahrq.gov/primer/culture-safety
Association of periOperative Registered Nurses. (2024). AORN Comprehensive Surgical Checklist Toolkit. Retrieved from AORN: https://www.aorn.org/guidelines-resources/tool-kits/comprehensive-surgical-checklist
Patient Safety Network . (2019, September 7). Wrong-Site, Wrong-Procedure, and Wrong-Patient Surgery. Retrieved from Agency for Healthcare Reseach and Quality: https://psnet.ahrq.gov/primer/wrong-site-wrong-procedure-and-wrong-patient-surgery
Shmerling, R. H. (2020, June 22). Harvard Health Blog First, do no harm. Retrieved from Harvard Health Publishing Harvard Medical School: https://www.health.harvard.edu/blog/first-do-no-harm-201510138421
The Joint Commission. (2024, May 15). Joint Commission Online-May 15, 2024. Retrieved from The Joint Commission: https://www.jointcommission.org/resources/news-and-multimedia/newsletters/newsletters/joint-commission-online/may-15-2024/
The Joint Commission. (2024, May 15). Sentinel Event Data 2023 Annual Review. Retrieved from The Joint Commission: https://www.jointcommission.org/resources/news-and-multimedia/newsletters/newsletters/joint-commission-online/may-15-2024/-/media/45c2f4a812c14f9fbc24cc22dcef8b3f.ashx
– Dawn Whiteside, DNP, MSN-Ed, RN, CNOR, NPD-BC, RNFA, is the director of education and professional development of the Competency & Credentialing Institute. She has over 35 years of experience as a perioperative nurse in many roles including circulator, scrub, first assistant, team leader, charge nurse, manager and educator.






